![]()

Indoff - offices nationwide
860-632-2026
860-632-2028 Fax
ahutton@ahutton.com
Below are Images that we have available for you to use on your hospital board. You can also supply your own or use our images.
Colors on Most Logos can be changed to your needs at no charge
Find By Letter=> A-B-C-D-E-F-G-H-I-J-K-L-M-N-O-P-Q-R-S-T-U-V-W-X-Y-Z
Additional Categories:
Washing Hands
Falling
Pain Management
Scale
Hourly
Rounding
Turning Schedule
Box Style
Dilation & Cervical
Effacement
See All Department Layouts here!
|
|
Activity -1 |

Activity - 2
|
|
 Activity 4
|
 Activity 5
|
Activity 7 |
 Activity 8 |
 Activity 9 |
 Activity 10 |
 Activity 11 |
 Activity 12 |
 Activity 13 |
 Activity 14 |
 Activity 15 |
Activity 18 |
 Activity 19 |
 Activity 20 |
 Activity 21 |
 Activity 22 |
 Activity 23 |
 Activity 24 |
 Activity 25 |
 Activity 26 |
 Activity 27 |
 Activity 28
|
Activity 29
|
Ambulance-1
|
|
Ambulance-2
|
Ambulance-3
|
Ambulance-4
|
 Ambulance 5 |
|
Ambulance 6
|
 Ambulance 7 |
 Ambulance 8 |
 Anesthesia 1
|
|
Anesthesia 2
|
Anesthesia 3
|
 Anesthesia 4 |
 Anesthesia 5 |
|
Anesthesia 6
|
|||
|
|
|
assistant-9
|
|
|
assistant-11
|
 Assistant- 19
|
Assistant 20 |
|
 Award-01 |
 award-2 |
 Award-03 |
|
 baby-1 |
 baby-2 |
 baby-3 |
 baby-4 |
 Baby-5 |
 baby-6 |
 baby-7 |
 baby-8 |
 Baby-9 |
 baby-10 |
|
 baby-12 |
 Baby-13 |
 baby-16-lactation |
 Baby-16-Solid |
 Baby 17 |
 Baby-20-car-seat |
 Baby-21 |
 baby-22 |
 Baby-23 |
 Baby-24 |
 baby-25 |
 Baby-27 |
 Baby-28 |
 Baby-29
|
 Baby-30
|
 Baby-31
|
 Baby-32
|
 Baby-33
|
 Baby-34
|
 Baby-35
|
 Baby 37
|
 Baby 38
|
 Baby 39
|
||
 Baby 40 |
 Baby 41 |
 Baby 42 |
 Baby 43 |
 Baby 44 |
 Baby 45 |
 Baby 46 |
 Baby 47 |
 Baby 48 |
 Baby 49 |
 Baby 50 |
 Baby 51 |
 Baby 52 |
 Baby 53 |
 Baby 54 |
 Baby 55 |
 Baby 56 |
 Baby 57 |
 Baby 58 |
 Baby 59 |
 Baby 60 |
 Baby 61 |
 Baby 62 |
 Baby 63 |
|
Baby 64
|
 Baby 65 |
Baby 66 |
 Baby 67 |
 Baby 68 |
 Baby 69 |
 Baby 70 |
 Baby 71 |
 Baby Toy 1 |
 Bathing-1
|
||
 Bed-1 |
 bed-2 |
|
|
 Bed-7 |
 Bed-12 |
 Bed 13
|
 Bed-14
|
 Bed-15
|
 Bed 16
|
 Bed 17
|
 Bed 18
|
|
Bed 19
|
 Bed 20 |
 Bed 21 |
 Bed 22 |
 Bedside Commode
|
 Birthdate-1
|
Birthdate 3
|
|
 Birth Certicate-1 |
 Birth Certicate-2 |
 Birth Certificate 3 |
 Birth Certificate 4
|
 Blood-1 |
Blood-2 |
Blood-3 |
 Blood-4
|
 Blood-5 |
 Blood-6 |
 Blood-7
|
 Blood 8 |
 Blood 9 |
 Blood 10 |
 Blood 11 |
 Blood 12 |
 Blood 14
|
 Blood 15 |
 Blood 16 |
 Blood 17 |
 Blood-18 Test |
|||
 Brain 2
|
Brain 3 |
Brain |
|
 Caduceus-16-Box |
|||
 Caduceus 29 |
caduceus-17
|
 Caduceus 27
|
 Caduceus 28 |
|
|
|
|
 Calendar-9-Box |
 Calendar-10
|
calendar-11
|
 Calendar-12 |
 Calendar-13 |
 Calendar-15 |
Caldendar-17 |
Calendar- 18
|
Calendar -19
|
 Calendar 20
|
calendar 21
|
 Calendar 22
|
 Calendar 23
|
 Calendar 24
|
 Calendar 25
|
 Calendar 26
|
 Calendar 27
|
 Calendar 28
|
 Calendar 29
|
 Calendar 30 |
 Call Button 1
|
| Fall Images are at Fall Images | |||

Call-light 1
|
 Call-Light 2
|
 Call-light 3
|

Call light 4 |
|
Call Light 5
|
 Caution-1
|
 Caution - 2
|
 Caution 3
|
 Caution 4 |
 Caution 5 |
 Caution 6 |
car-1
|
|
Car 2
|
 Case Manager 1
|
 Case Manager 2
|
 Case Manager 3
|
 Case Manager 4
|
 Case Manager 5 |
 CAT Scan-1 see CT |
|
|
Catering-1
|
Catering 2
|
||
 Catering 3
|
 Catering 4
|
 Cell Phone-1 |
 Chair 1 |
 Cell-Phone 2 |
 Checkout time-1 We can change the time displayed! |
 clipboard-1
|
 clipboard-2 |
 clipbord-3 |
 Clipboard 4 |
clipboard-5
|
 Clipboard-6
|
 Clipboard-7 |
 Clipboard-8
|
 Clipboard-9
|
Clipboard-10
|
 Clipboard-11
|
 Clipboard 12
|
 Clipboard 13
|
 Clipboard 14
|
 Clipboard 15
|
 Clipboard 16
|
 Clipboard 17
|
 Clipboard 18 |
|
Clipboard 19
|
 Clipboard 20 |
 Clipboard 21 |
 Clipboard 22 |
|
Clipboard 23
|
Clock 1
|
Clock 2
|
|
 Compass-1
|
 Compass-3
|
Compass-4
|
 Compass-5
|
|
Consultation-1
|
Consultation-2 |
 Consult-3 |
 Consultation-4 |
 Consultation-5
|
Consultation-6
|
Consultation-7
|
Consultation-8 |
|
Counseling-1
|
Counseling-2
|
Counseling-3
|
Counseling-4
|

counseling-5
|
Counseling-6
|
CNA-1
|
|
 cross-2 |
 Cross-3
|
 Cover your mouth
|
CT Scan 1 |
 Discharge - 1 |
 Dentures-1 |
 Dentures-2 |
 Dentures-4 |
 Design 1
|
 Design 2
|
 Diagnosis 1
|
|
 Diet-baby |
 Diet-2
|
|
Diet 4 |
 Diet 5 |
 Diet 6 |
Diet 7 |
 Diet 8 |
|
Dilation and Cervical Effacement |
DNR-1
|
DNR-2
|
|
 DNR 6
|
DNR 7 (full code)
|
 Doctor-1 |
 Doctor-2 |
 doctors-3 |
 doctor-4
|
 doctor-5 |
|
 doctor-9 |
 Doctor-10 |
 Doctor-11 |
 doctor-12 |
 doctor-13 |
 doctor-16 |
 doctor-17 |
 Doctor-18 |
 Doctor-19 |
 Doctor-20 |
 Doctor-21 |
 doctor-22 |
 doctor-23 |
 doctor-24 |
 Doctor-25 |
|
 doctor-27 |
 Doctor-28 |
 Doctor-29 |
 Doctor-30 |
 Doctor-31 |
 Doctor-32 |
 Doctor-33 |
 Doctor-34 |
 Doctor-36 |
 Doctor-37 |
 Doctor-38 |
 Doctor-39 |
 Doctor 41
|
 Doctor 42 |
 Doctor 43 |
 Doctor 45 |
 Doctor 46 |
 Doctor 47 |
 Doctor 48 |
 Doctor 49 |
 Doctor 50 |
 Doctor 51 |
 Doctor 52 |
 Doctor 53 |
|
Doctor 54
|
 Doctor 55 |
 Doctor 56 |
|
 Doctor-heart
|
 doctor-patient-1 |
 doctor-patient-2 |
 Doctor-patient-5 |
 doctor-nurse-patient-1 |
 don't walk-1 |
|
 Dressing-1 |
 education-1 |
 Education 2 |
Education 3 |
 Education 4 |
 Education 5 |
 Education 6 |
 Education 7 |
 Edcuation 8
|
 EKG 1
|
|||
|
EKG 2
|
 EKG 3 |
Emergency 1
|
EMT logo
|
 EMT-1 |
|
 EMT-3 |
EMT 4
|
|
EMT 5
|
EMT 6
|
EMT 7
|
EMT 8
|
|
exam-1
|
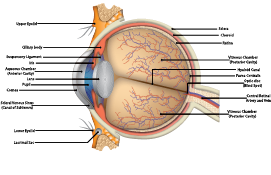
Eye- Anatomy |
 Eye 1 |
|
 For all Falling images click here |
For Falling Click |
 Family-1
|
|
 Family-2
|
|
Family-6
|
 Family-9
|

Family - 10
|
 Family - 11
|
 Family 12 |
 Family 13 |
|
Family 14
|
 Family 15 |
Family 16 |
Family 17 |
 Family 18 |
 Family 19 |
 First-Aid-1
|
 First-Aid-2
|
 First-Aid-3
|
|
|
 First Aid 6 |
 First Aid 7 |
 First Aid 8 |
 First Aid 9 |
 First Aid 10 |
 First Aid 11
|
 First Aid 12 |
 First Aid 13 |
|
 Food-1 |
 Food-2
|
 Food-3
|
 Food-4
|
 Food-5
|
 Food-6
|
 Food-7
|
Food 9 |
 Food 10 |
 Food 11 |
 Food 12 |
 Food 13 |
|
|
 fork-knife-1-box |
 Fork-knife - 2 |
 fork-knife-3 |
 fork-knife-4-green |
 ForkKnife-4-red
|
|
Fork-knife -7 |
|
Fork Knife 8 |
 Fork Knife 9 |
|
|
 Guerney-1
|
 glasses-01 |
|
|
 Glasses-4
|
 Glasses- 6
|
 Glasses 7 |
Glasses 8
|
|
Goal-1
|
 Goal-2 |
Goal-4
|
|
 Goal - 5
|
 Goal- 6
|
Goal 7
|
Hair 1
|
 hearing-01
|
|
 hearing-03 |
|
|
hearing-05
|
 hearing-06
|
|
 Hearing-8
|
|
Hearing 9 |
 Hearing 10 |
 Hearing 11 |
 Hearing 12 |
 Hearing 13 |
Hearing 14
|
 Hearing 15 |
|
 heart-1
|
 heart-2 |
 Heart-3 |
 Heart-4 |
 Heart-5 |
 Heart-6 |
Heart-7 |
Heart-8 |
|
Heart-9 |
Heart- 10 |
Heart 11 |
Heart 12 |
|
.
Heart 13 |
Heart 14
|
Heart 15 |
Heart 16 |
|
Heart 17 |
Heart 18
|
Heart 19 |
 Heart 20 |
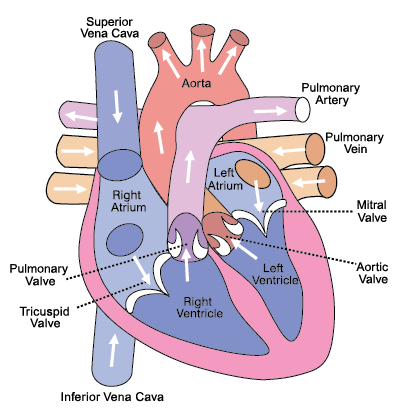 Heart-diagram-1
|
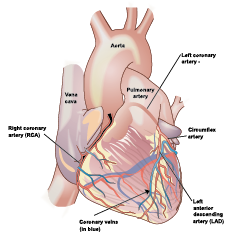 Heart-diagram-2
|
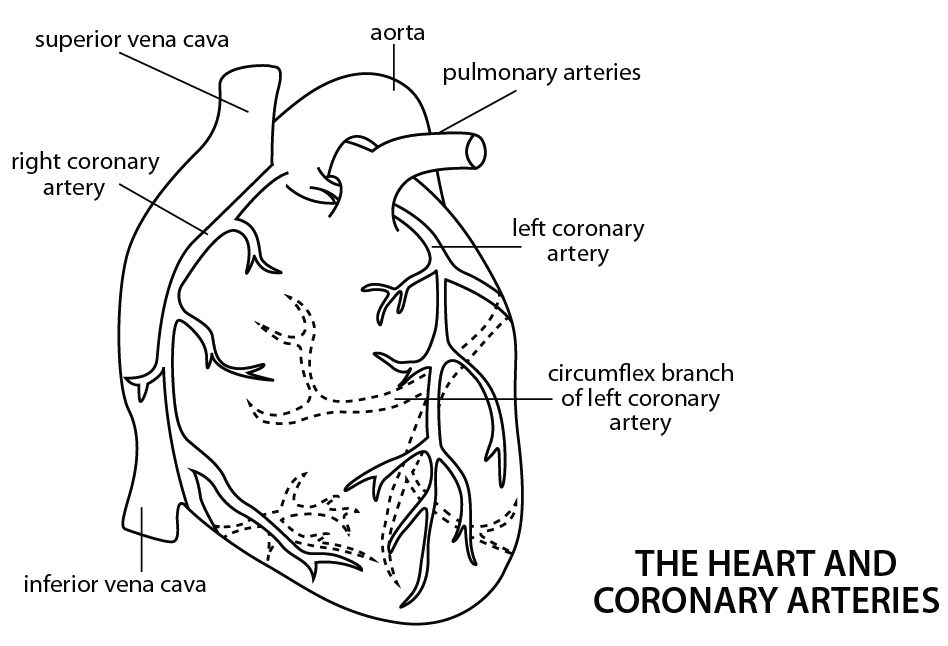
Heart-diagram-3
|
Home-1
|
|
|
 Home-3 |
 Home-4 |
 Home-5 |
|
|
 Home-7 |
 hOME-8 |
Home-9 |
|
|
Home 11 |
Home 12 |
 Home 13 |
|
Home 14
|
Home 15 |
||
 Hospital-1 |
 Hospital 2 |
 Hospital 3 |
|
|
Hospital 4 |
Hospital Cross-01
|
|
|
|
|
 housekeeper-1 |
 Housekeeper-1-color |
|
 Housekeeper-8 |
 Housekeeper--9 |
 Housekeeper-10 |
|
|
|
|
 housekeeper-14 |
|
|
|
|
|
Housekeeping-19
|
 Housekeeping 20 |
 Housekeeping 21 |
Housekeeping 22 |
Housekeeping 23 |
 Housekeeping 24 |
 Housekeeping 25 |
Housekeeping 26
|
|
 Hospitality-1 |
ICU-1
|
 Imaging-1 |
|
 information-1 |
Information-2
|
|
|
|
|
 INFORMATION-7 |
Information-8
|
Information 9 |
|
Information 10
|
Information 11
|
||
|
|
Intake 1
|
 Intake 2 |
 Intake 3 |
|
Intake 4 |
Interpreter-1 |
 Interpreter-2-box |
 Intestine-1 |
|
IV-1
|
IV 2 |
 IV 3 |
 IV 4 |
|
IV 5 |
Instruments-1 |
|
Jersey-1 |
|
Jersey-2
|
 Jersey-3 OK to change letters and colors
|
Kidney-1
|
 Kidney 2 |
 Kidney 3 |
 Kidney 4 |
Language-1
|
Language 2
|
|
Language 3
|
 Language 4
|
 Language 5 |
Liver 1
|
 Lung-1
|
 Lungs 2 |
 maid-1 |
 maid-2 |
 maid-3 |
|
 Maintenance 2 |
Maintenance 3 |
|
Maintenance 4
|
 Maintenance 5 |
 Maintenance 6 |
 Maintenance 7 |
 Mask-1 |
 Medical-1 |
||
 Medical-2 |
medical-button-green-1 |
 medical-button-red-1
|
 medical-button-blue-1
|
 medical-button-yellow-1
|
 medicine-1 |
 Meeting 1 |
Mouth 1
|
|
Mouth 2
|
 No Smoking 2 |
||
 Notes 1 |
 Notes 2 |
 nurse-1-Hat |
Nurse 2
|
|
Nurse 3 |
|
Nurse-8
|
|
|
|
Nurse-21
|
|
Nurse-24
|
|
Nurse-26
|
|
Nurse-32
|
|
 Nurse-34 |
|
|
Nurse 42 |
 Nurse-43 |
 Nurse-44
|
 Nurse-45
|
Nurse 46
|
 Nurse- 51
|
 Nurse 52 |
 Nurse 53 |
 Nurse 54 |
 Nurse 55 |
 Nurse 56 |
 Nurse 57 |
 Nurse 58 |
 Nurse 59 |
 Nurse 60 |
 Nurse 61 |
 Nurse 62 |
|
Nurse 63
|
Nurse 64
|
 Nurse 65 |
 Nurse
66 Nurse
66 |
 Nurse
67 Nurse
67 |
 Hurse-68 |
 Nurse-69 |
 Nurse-70 |
|
|
 nurse-assistant-02-yellow |
 Nurse-assistant-6-BOX |
|
|
Nurse Assistant 8
|
 Nurse Assistant 9
|
Nurse Assistant 10
|
Nurse Assistant 11
|
|
Nurse Assistant 12
|
 Nurse Assistant-14 |
 Nurse Assistant 13 |
 Oxygen-1
|
 Other-partners
|
|
||
 patient-01 |
 Patient-02
|
 Patient 3 |
 Patient 4 |
 Patient 5 |
|
Phone -1
|
 Phone-2 |
|
|
 Phone-4-box |
|
 Phone-6 |
 Phone-7 |
 Phone-8 |
 Phone-9 |
 Phone-10 |
 Phone-11 |
 Phone-12 |
 Phone-13 |
 Phone-14 |
 Phone-17 |
 Phone-19 |
Phone 22 |
 Phone 23
|
 Phone 24
|
 Phone 25
|
 Phone 26
|
 Phone 27
|
 Phone 28
|
 Phone 29
|
 Phone 30
|
 Phone 31
|
|
Phone 32
|
 Phone 33
|
 Phone 34 |
 Photo-1 |
|
|
|
 PA-2 Physician Assistant |
|
 Planning 1 |
 Planning 2 |
 Planning 3 |
 Planning 4 |
 Planning 5 |
 Planning
6 Planning
6 |
 Praying-1 |
 Praying-2 |
 Precautions 2 |
 Precautions 1
|
 Procedure 1 |
|
 Professional-2 |
 Professional-6 |
 Professional-9 |
 Professional-10 |
 Professional-11 |
 professional-13 |
 professional-14 |
|
 professional-17 |
 professional-18 |
 Professional-19
|
Prosfessional-20 |
|
professional-21
|
 professional-22
|
|
|
|
|
 professsional-27 |
 professsional-28 |
|
|
professional-30
|
professsional-34
|
professsional-35
|
 Professional-36 |
|
Professional-38
|
Professional-39
|
Professional-40
|
Professional-43
|
 Puppy-1 |
|
 Question-2 |
|
|
|
 Question-4-Box |
|
 Question-6 |
 Question-7 |
 Question-8
|
 Question 10
|
 Question 11 |
|
Question 12
|
Question 13 |
Question 14 |
Question 15 |
 question-button-blue-1
|
question-button-green-1
|
question-button-red-1
|
question-button-yellow-1
|
 Question Fam - 1
|
 Rounding-1
|
||
 Respiratory-01 |
|
 Respiratory-3 |
 Respiratory-6
|
 Respiratory-7 |
 Respiratory-8 |
 Respiratory-9 |
 Respiratory-02-Box |
 Respiratory-10 |
 Respiratory-12 |
 Respiratory 13
|
 Respiratory 14
|
 Respiratory 15
|
 . .Respiratory 16
|
 Respiratory 17
|
 Respiratory 18 |
|
|
 RX-8 |
||
 RX-10 |
|
 RX-12
|
 Rx-13 |
 RX-13-box |
 RX-14 |
RX-15 |
RX-17 |
 RX-18
|
RX 19 |
RX 20 |
RX 21 |
 RX 22 |
RX 23
|
RX 24 |
RX 25 |
|
RX 26
|
RX 27 |
RX 28
|
RX 29 |
|
RX 30 |
RX 31
|
RX 32 |
RX 33 |
|
RX 34
|
RX 35 |
RX 36 |
RX 37 |
 RX 38 |
RX 39 |
RX 40 |
|
|
|
|
Safety 1 |
|
 Safety 2
|
|
|
 Scale 4 |
 Scale 5 |
Scale 6 |
Scale 7
|
Scale-8 |
 Security-1
|
|
|
|
 Smile4 |
Smile 6
|
Shower-1 |
Shower-2 |
 Smiley-pain |
|
|
 Smiley-Respiratory |

|
|
Smiley-Bath |
 Smiley - 1
|
 Social Worker 1 |
specimen-5
|
specimen-6
|
Stomach 1
|
|
Stomach 2
|
 Stomach 3 |
||
|
Stop-5
|
Stop-6
|
stop-8
|
 Stop-9 |
|
Stop 10
|
Stop 14
|
 Slight Light 1 (yellow)
|
Stop Light 2 (Red)
|
|
Support 1
|
|
|
|
 Surgery-5 |
Surgery 6
|
Surgery 7
|
 Surgery 8 |
 Surgery-9-Fire-Ignition Source |
 Surprise-1 |
 Surprise-2 |
|
|
Team-1 |
Tech-1 |
|
 Tech-3 |
|
|
|
 Test-6 |
|
|
|
|
|
 Tests-13
|
 Tests-14
|
Tests-15
|
 Tests 16
|

Tests 17
|

Tests 18
|
 Tests 19
|
 Tests 20 |
Tests 21
|
|
Tests 22
|
 Tests 23
|
 Tests 24 |
 Test 25 |
 Tests 26 |
 Tests 27 |
Tests 28
|
Tests 29
|
 Tests 30 |
 Tests 31 |
Tests 32
|
|
|
Toilet-1
|
|||
|
|
|
therapy-1 |
 therapy-2 |
|
|
Therepy-4-box
|
|
|
 Therapy-08 |
 Therapy-09 |
 Therapy-10 |
 Thereapy-11 |
 Therapy-12
|
 Therapy-13 |
 Therepy-14 |
Therepy-16
|
|
|
 Therapy-20 |
 Therapy-21 |
 Therapy-22 |
|
Therapy-25 |
 Therapy-26 |
Therapy 27 |
Therapy 28 |
|
Therapy 29
|
Therapy 30 |
Therapy 31 |
Therapy 32 |
|
Therapy 33
|
Therapy 34 |
Therapy 35 |
Therapy 36 |
|
Thermometer 1 |
Thermometer 2
|
||
|
Thermometer 3
|
Thermometer 4
|
Thermometer 5 |

Time 1
|
|
Time-2
|
Time-4 |
Time-5
|
|
|
Time - 10
|
Time 11
|
|
|
 to-do-list-1 |
|
to-do-3
|
|
|
to-do-4
|
 Time-out-1 |
|
|
|
|
 time-out-5 |
|
 TV 1 |
 TV 2 |
 TV 3 |
TV 4
|
|
|
|
Tubing-1
|
Urine-cup 1
|
Urine Cup 2
|
|
|
 Walking-2-Box |
|
Water-2
|
|
Water-3
|
 Water-5 |
|
Water-7
|
 Weather-1 |
 Weather-2 |
 Weather-3 |
 Weather-4 |
 Weather-5 |
|||
|
Walker-1
|
Walker-2
|
 Walker -3 |
|
|
|
 wheelchair-1
|
wheelchair-2
|
Wheelchair 3 |
 Wheelchair-4 |
|||
|
Wi-Fi 1
|
X Ray 1
|
X Ray 2
|
X Ray 3
|
|
X Ray 4
|
 X Ray 5 |
|
|

































































































 .
.



























































































































 .
.





























































































 Water-6
Water-6








And, don't forget: we can print custom phone numbers and room numbers per board!
New Limited English Proficiency Requirement!!!
Do You have Patients that speak many languages?
see also => Ideas for Hospital Boards